This is pediatrics history taking model 6 months old female child was presented with chief complaints of cough and fever. Here is the history of this case.
Quick Navigation
Pediatrics History Taking
Name: ***** ********
Age: 6 months
Sex: female
Address: ********** *******
Mode of admission: via Emergency
Date of admission: 2021-05-22
Informant: mother
Name: **** *****
Occupation: Teacher
Education: up to Bachelor’s level
History is reliable.
* name of patient, informant and address are hidden for privacy of the patient.
Chief complaints:
Cough 15 days back.
Fever for 9 days.
History of present illness:
According to the informant, she was apparently well 16 days back and she developed cough which was insidious in origin, paroxysmal, increasing in night and during lying and feeding. Cough was associated with noisy breathing, running nose, difficulty in breathing, subcostal retractions and increased respiratory rate.
Fever was insidious in onset, intermittent, not documented, high grade, on and off type, had diurnal variation and relieved on medications.
No history of rigor, rashes, nasal congestion.
No high-pitched cry, irritability, photophobia, fainting, cry during feeding.
No abnormal body movements.
No increased seating in forehead, puffiness of face, sacral edema.
No increased precordial activities, cyanosis, no suck-rest-suck cycle.
No cry during micturition, normal urination, no abnormal urine color.
No hematemesis, vomiting, loose stool, melena, color of stool was yellow.
Medication history:
Total 7 drugs, 4 of them are IV (mixed with normal saline), 2 oral and one inhaled. No oxygen given.
Past history:
No history of similar episode in past, no neonatal jaundice, no difficulty in breastfeeding in past.
Birth history:
Antenatal:
1st trimester:
Spontaneous conception, Total 3 antenatal check visits, received folic acid, blood tests and USG done, no excessive vomiting, vitals and investigations were at between normal range.
2nd trimester:
Quickening perceived at 5th month and were more than 10 fetal movements per day, 3 antenatal visits, Iron, calcium taken, USG done and shown no any fetal anomalies, taken single dose of Tetanus toxoid, vitals and investigations were at between normal range. No UTI, preeclampsia, gestational diabetes.
3rd trimester:
Taken iron and calcium, continued perceiving fetal movements, 3 antenatal visits. No history of eclampsia and other complications, no fainting attacks.
Natal:
Booked delivery, Normal vaginal delivery, term baby, spontaneous cry.
Post-natal:
Birth weight was 3.1 kg, no NICU stay, no other complications to mother, 1 day of hospital stay, immunized according to national schedule.
Developmental history:
Holds neck, stands on support, shares toy, plays with objects, playful, approaches objects with one hand.
Dietary history:
breastfed, bottle feed due to low milk ejection.
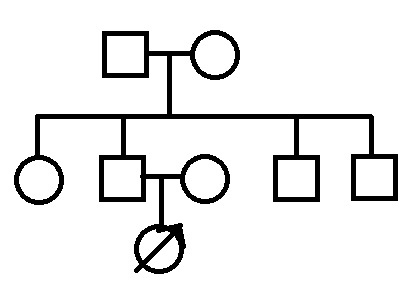
Family history:
Socioeconomic history:
There are 5 members in family, 2 of them are earning members. The house is paucca, 4 rooms with proper ventilation, separate kitchen and toilet. Use water from tap and cook food in gas.
Per capita income: ****** $

